Enabling Environment
Non-invasive and Unrestrained Monitoring of Human Respiratory System by Sensorized Environment
Abstract
This report describes a living-space-shaped system for non-invasively
and unrestrainedly monitoring the human respiratory system and intelligibly
reporting its results. This environmental system consists of sensorized furniture:
1) a ceiling dome microphone, 2) a pressure sensor bed, and 3) a washstand display.
The ceiling dome microphone consists of a ceiling dome, a lighting fixture,
and an omnidirectional microphone. The ceiling dome microphone can detect not
only snoring sounds but also normal breathing sounds, i.e., airflow at the mouth
and nose. The pressure sensor bed has 210 tactile sensors and can monitor body
movement, breath curve and posture. By analyzing the breath curve, the system
can estimate oxygen desaturation frequency. By integrating the above functions,
for example, the system can find obstructive apnea, which is a typical apnea
such that the patient cannot inhale the air despite of breath effort and that
the concentration of the oxygen in blood falls. The washstand display can provide
information related to the conditions of the respiratory system in the personüfs
daily life. To prove the effectiveness of the integrated system, experiments
are conducted for a patient suffering from breath disorder.
INTRODUCTION
Daily living space works to enable our lives. Engineering
on daily living space enables to improve and augment human support functions
in our daily living spaces through analyzing implicit functions based on careful
observation of the spaces, characterizing them in an explicit form, clarifying
functions to be improved and augmented, realizing the desired functions by engineering
components, and finally integrating the realized function into the daily living
space in a natural form. Daily personal healthcare support at home is one of
the most necessary functions our daily living space should have in a near future.
To realize such a function in socially acceptable form, an unrestrained and
non-invasive means of observing physiological status is the key technology.
This report describes a sensorized environment for non-invasively and unrestrainedly
monitoring the human respiratory system. The environment consists of a sensing
part for robustly and naturally observing inhabitants, 2) a digital human model
for understanding conditions of the human respiratory system
from observed data, and 3) a presenting part for letting them utilize understood
information.
NON-INVASIVEANDUNRESTRAINED MONITORING BY SENSORIZED LIVING
SPACE
The human respiratory system is very complex. Therefore, it requires monitoring
with many sensors such as pressure sensors to monitor the chest and abdomenüfs
movement, thereto for airflow around the nose and mouth, a contact-type of
microphone for snoring, oximeters for oxygen saturation, and mercury sensors
for posture(Fig. 1 (B)). Since these sensors need to be attached directly
to the person, they impose much physiological or mental burden on him or her.

Figure 1: Environment Sensorization
Indeed, the conventional contact-type sensors can monitor physiological values
certainly as long as they are used adequately. Actually, however, they very
often fail to monitor continuously. For example, in 48 percent of the cases
(21 of 43 cases) in the clinical study the authors conducted, the monitoring
system failed to measure the physiological values continuously enough to diagnose
disease. This suggests that even in a hospital where more priority is given
to accurate monitoring than to comfortable monitoring, non-invasive and unrestrained
monitoring is required to minimize this failure. The developed living space,
SELF (Sensorized Environment for LiFe) is sensorized as shown in Fig. 1. In
this study, sensorization meansmaking the room itself a sensor for inputting
human daily behavior by embedding sensors into the room invisibly to keep
the roomüfs appearance natural and maintain its original function. The figure
explains main components of the typical conventional computers are transformed
to the room. For example, a keyboard, which is a kind of touch sensor, becomes
a bed-shaped touch sensor. A microphone is embedded into a lighting fixture.
A display is embedded into a washstand. Figure 1 (C) shows the photograph
of the constructed bed room. SELF support daily healthcare at home as follows:
1) SELF observes a person using the pressure sensor bed and the ceiling dome
microphone when he or she goes to bed and sleeps, 2) SELF reports useful information
to the person using the washstand display when he or she goes to the washstand
typically after waking up or before going to bed.
ENVIRONMENT SENSORIZATION
This section describes a pressure sensor bed and a ceiling dome microphone
as an example of the sensorized environment. Sensors are embedded in both
systems invisibly.
Pressure sensor bed
The pressure sensor bed consists of a pressure distribution sensor array,
a controller, and a bed. The pressure distribution sensor has 210 Force
Sensing Resistors (FSRs) which are set at 7[cm] intervals. An FSR is a thin
film sensor made from piezoresistive polymer. The sampling frequency of
the pressure image is 20 [Hz]. The measuring range of each pressure sensor
is 0 to 1[kg]. The pressure sensor bed is used for monitoring the breath
curve, oxygen desaturation(*1) frequency, posture,
and body movement.
Based on the fact that Cheyne-Stokes-like breathing occur at high probability
in oxygen desaturation, the pressure sensor bed can estimate oxygen desaturation
frequency by measuring Cheyne-Stokes-like breathing(*2)
frequency. Figure 2 comparesthe frequency of Cheyne-Stokes-like breathing
and oxygen desaturation 4%(*3) at an interval
of 10 minutes with 3 patients with disease of different seriousness.
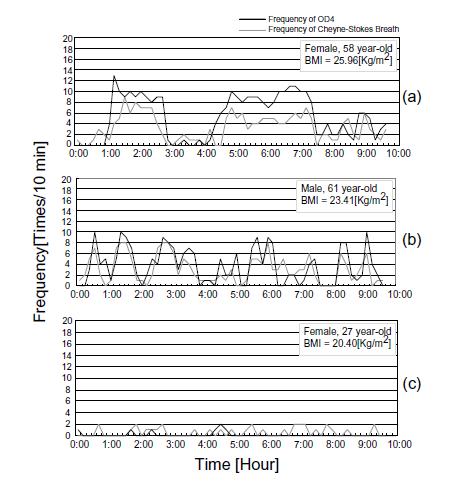
Figure 2. Comparison of histogram of Oxygen desaturation 4% (OD4)
detected by conventional sensor and Cheyne-Stokes-like breathing detected
by pressure sensor bed
(*1) Oxygen saturation (SpO2) expresses the
percentage of oxyhemoglobin molecules to all hemoglobin molecules and is
almost 100 % in healthy subjects. Oxygen desaturation means the percentage
falls for some reasons. Doctors find oxygen saturation monitoring important
physiologically to judge whether respiration is normal.
(*2) It is a kind of periodic respiration.
The authors defined Cheyne-Stokes-like breathing as the breath with respiration
effort without ventilation accompanying gradual increase and gradual decrease,
or sudden increase and gradual decrease.
(*3) Oxygen desaturation 4% means oxygen
saturation falls 4%. From Fig. 2, a high correlation was confirmed between
the Cheyne-Stokes index monitored by the pressure sensor bed and oxygen
desaturation 4% index.
Ceiling dome microphone
The authors invented the ceiling dome microphone which consists of a ceiling
dome, a lighting fixture, and a omnidirectional microphone. This device
has two functions: indirect lighting and gathering sound. The ceiling dome
is used to reflect both light and sound. A microphone is set at the focal
point of the reflector. The diameter of the dome is 900[mm]. The device
enables detection not only snoring sounds but also normal breathing sounds
with high sensitivity while keeping the roomüfs appearance natural. It is
positioned above the bed. The gain obtained by the ceiling dome is maintained
at more than 20[dB] for high frequency sounds of more than 6[kHz]. Since
the frequency of normal breathing sounds ranges from 5 to 15 [kHz], this
device can detect breathing sounds, i.e., air flow at the mouth and nose.
Figure 3 shows an example of breathing sounds detection using the ceiling
dome microphone. Roomüfs background noise includes such noises as those of
an air conditioner and a computer. The figure shows that both the inhalation
and exhalation component of the breath cycle are detected quite clearly.
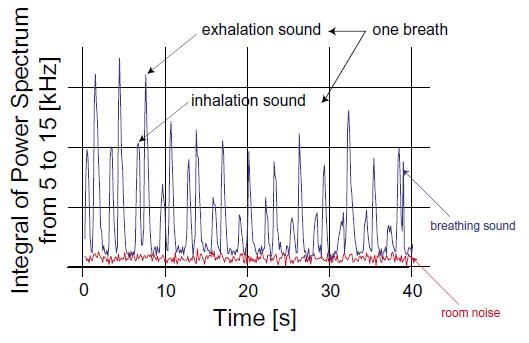
Figure 3. Detection of normal breathing sounds by ceiling dome microphone
UNDERSTANDING INTERNAL STATUS BASED ON A MODEL OF HUMAN FUNCTIONS
Human respiratory system
Figure 4 shows physiology and physics of human respiration, and a method
for monitoring conditions of the human respiratory system. The human respiratory
system deeply relates to brain activity, the circulatory system, respiratory
organs such as lung, respiratory muscles such as diaphragm, peripheral organs
such as nasal cavity and oral cavity, human posture and so forth as shown
in Fig. 4 a). To monitor conditions of the human respiratory system, a model
of the respiratory system for estimating the conditions from sensor data
is necessary. This section describes the developed model of the human respiratory
system and a method of estimating the conditions using the model.
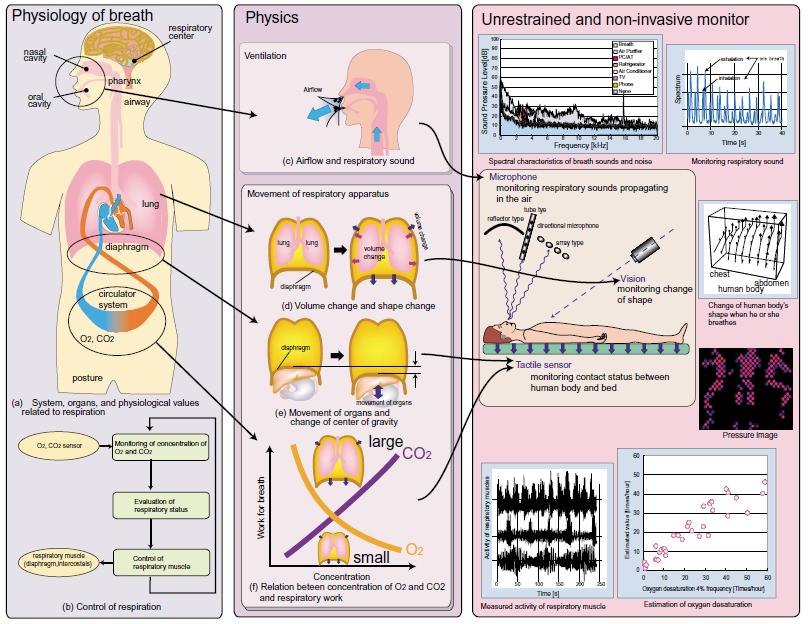
Figure 4. Physiology, physics and measuring method of human respiratory
system
Physiology of human respiratory system
Respiration keeps oxygen and carbon dioxide in body fluids within a constant range.
Tidal air is controlled by respiratory muscles such as the diaphragm and
intercostals based on the oxygen and carbon dioxide concentration detected
by some internal sensors. The sensors exist in carotid body of the common
carotid artery and central chemosensitive area of the medulla oblongata.
The control of the human respiratory system is shown in Fig. 4 b).
Non-invasive and unrestrained monitoring of human respiratory system
The followings are physiological values that the developed
human model can estimate from sensor data. Physics of the human respiratory
system and the methods for monitoring these physical values are outlined
in Fig. 4.
- Posture, body movement
Posture is recognized by analyzing pressure sensor signals based on a posture
model. Body movement is calculated by detecting changes in pressure sensor
output.
- Breath curve
Breath curve is calculated by the "same phase sum method" which
is a method for appropriately summing the control offset considering the
phase difference in the output change in the pressure sensor.
- Oxygen desaturation in blood
Oxygen desaturation is detected by detecting Cheyne-Stokes-like breathing
from the calculated breath curve. The principle is that Cheyne-Stokes-like
breathing occurs with high probability when oxygen desaturation appears.
This method can detect only the frequency of oxygen desaturation, not absolute
values of oxygen desaturation.
- Airflow at mouth and nose
Airflow at the mouth and nose is detected using the ceiling dome microphone.
Evaluation of estimation function of SELF
The authors conducted experiments for a real patient suffering from Sleep
Apnea Syndrome. Figure 5 compares physiological values measured by a conventional
system and that estimated by the developed system. Apnea estimation by our
system is done using both a detecting function of snoring sounds and a monitoring
function of the amplitude of breath curve. If the amplitude is less than
a certain threshold and that there are no snoring/breathing sounds, the
system finds obstructive apnea. Obstructive apnea is a typical apnea such
that the patient cannot inhale the air despite of breath effort and that
the concentration of the oxygen in blood falls. Oxygen desaturation estimation
is done by analyzing the change of the amplitude of breath curve. The figure
shows the system can estimate apnea correctly in 8 of 10 cases. The figure
also shows the system can estimate ogygen desaturation in 9 of 10 cases.

Figure 5. Comparison monitoring and estimating function of SELF with
conventional one
PRESENTING ENVIRONMENT
This section reports a washstand display as an examples of an information
providing furniture. The washstand tends to be used every morning and night,
which means if the washstand has a function of providing information as well
as mirroring the inhabitant, it is able to convey periodically. According
to questionnaire survey conducted by us, women spend at the washstand from
30 minutes to 1 hour a day. Since there are enough time to read information
from the washstand, the washstand is one of the most suitable place for providing
a person with useful information. Figure 6 shows the developed washstand display.
It consists of a liquid crystal display (LCD) having a touch sensor and a
vision system. The LCD is used for displaying not only a personüfs face but
also some health information analyzed by SELF.
Figure 7 shows the image displayed on the LCD. The health information is displayed
around the face. This report consists of weekly and daily information on the
changes in health condition and is expressed with bar graphs and text. Changes
to be notified to the person are determined based on the average condition
of the person and of other people. For the basis of information on the average
condition of people, we used a medical textbook.

Figure 6. Constructed washstand display

Figure 7. Example of output of washstand display
CONCLUSION
This report describes a sensorized environment for non-invasive and unrestrained
monitoring the human respiratory system.The system consists of 1) a sensorized
environment for robustly and naturally observing inhabitants, 2) a human model
for understanding conditions of the human respiratory system, and 3) a presenting
environment for letting them utilize analyzed information. As examples of
the sensing and presenting environment, this report reports the daily living
space (SELF) which has a ceiling dome microphone, a pressure sensor bed, and
a washstand display. The experiments conducted for a real patient suffering
from Sleep Apnea Syndrome proved the developed system can estimate apnea,
oxygen desaturation frequency using sensory data from the pressure sensor
bed and the ceiling dome microphone.
References
- Y. Nishida, T. Hori, "Non-invasive and Unrestrained Monitoring of Human
Respiratory System by Sensorized Environment, " Proc. of the First IEEE
International Conference on Sensors (Sensor 2002), pp. 62.4(1)-(6), June 2002
- T. Kuga, M. Takayama, T. Ishii, Y. Nishida, "Respiration monitoring
of sleep apnea syndrome using a pressure sensor bed," ī¹ł¶ē╚, Vol. 13, No.
2, pp.1-11, 2001
- Y. Nishida, T. Hori, "Sensorized Living Space with a Model of Human
Functions," Proc. of Digital Human Modeling Workshop at IEEE International
Conference on Intelligent Robots and Systems (IROS2001), 2001
- Y. Nishida, T. Hori, T. Suehiro, S. Hirai, "Sensorized Environment
for Self-communication Based on Observation of Daily Human Behavior,"
Proc. of 2000 IEEE/RSJ International Conference on Intelligent Robots and
Systems (IROS2000), pp.1364-1372, 2000
- Y. Nishida, T. Hori, T. Suehiro, S. Hirai, "Monitoring of Breath Sound
under Daily Environment by Ceiling Dome Microphone," Proc. of 2000 IEEE
International Conference on Systems, Man, and Cybernetics (SMC2000), pp.1822-1829,
2000